
C3R Treatment
What is Keratoconus & C3R Corneal Cross Linking Treatment | केरेटोकोनस का इलाज
Welcome to Bansal Eye Hospital. BEH is the pioneer eye hospital in North India and one of the Best Eye Hospital in Chandigarh. Bansal Eye Hospital is empanelled with Haryana Government, Himachal Government, Punjab Government, ESIC- Himachal Pradesh, CGHS, ECHS for Lasik Laser Eye Surgery, Specs Removal Surgery, C3R Surgery, Cataract (Safed Motia or Motiabind) Surgery, Diabetic Retinopathy, Glaucoma (kala motia) and other eye related treatment and surgery.

What is keratoconus?
Keratoconus is a common bilateral corneal condition, occurring in more than 1 in 1000 people. The condition typically starts in adolescence and early adulthood.
Usually one eye is involved more than the other. Infrequently it may occur only in one eye.Keratoconus is a disease with an uncertain cause, and its progression following diagnosis is unpredictable. It is more common in people with allergies or those who rub a_imagetheir eyes frequently. If afflicting both eyes, the deterioration in vision can affect the patient’s ability to drive a car or read normal print. Further progression of the disease may lead to a need for surgery.
Despite its uncertainties, keratoconus can be successfully managed with a variety of clinical and surgical techniques, and often with little or no impairment to the patient’s quality of life.
KERATOCONUS (FROM GREEK: KERATO- HORN, CORNEA; AND KONOS CONE)
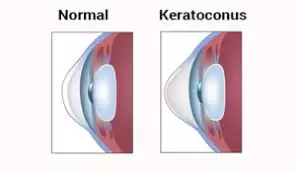
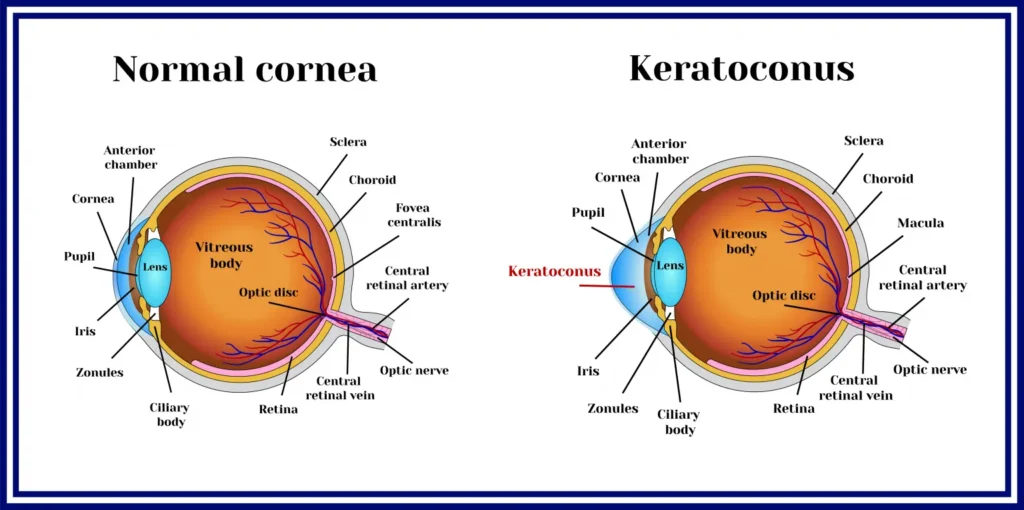
The cornea is the clear window on the front of the eye. It is usually a regular spherical dome in shape. The substance of the cornea consists of hundreds of layers that are linked to each other by a substance called collagen. If these collagen cross-links between layers are lost due to keratoconus, there is a progressive corneal thinning and stretching which gradually progresses, often in both eyes.
Normal pressure within the eye causes the cornea to bulge forward into an irregular cone shape. When light enters the eye, it first passes through the cornea. If the cornea has turned conical, there is distortion of the image. The eye develops astigmatism (cylindrical errors) and myopia [shortsightedness] and the vision may become severely blurred.
A simulation of the multiple images seen by a person with keratoconus.
Keratoconus: Causes, Symptoms, Diagnosis, Risk and Treatment
Risk factors
Reported risk factors for keratoconus include eye rubbing, a family history of keratoconus, genetic predisposition, certain systemic disorders such as Down’s syndrome, ocular allergy, connective tissue disease, and long-term rigid contact lens wear. It is usually an inherited corneal disorder, often in an autosomal dominant fashion. This means that approximately 50% of family members may end up with it. But it also can be random with no other family members affected. It affects men and women in equal proportions and is bilateral in 90% of patients.
Keratoconus symptoms and signs

Diagnosis
His is usually done by an ophthalmologist with a detailed eye examination. Diagnosing early keratoconus can be tricky, since mild disease often does not show any identifiable signs on slit-lamp examination; however, recent and a more definitive diagnosis can be obtained using corneal topography, in which an automated instrument projects an illuminated pattern onto the cornea and determines its shape from analysis of a digital image. The topographical map reveals distortions or scarring in the cornea, with keratoconus revealed by a characteristic steepness of curvature which is usually below or around the centre of the cornea. The topography record of the degree and extent of the deformation is used for assessing its rate of progression. Unilateral cases tend to be uncommon. Sometimes it’s a mild condition in the better eye, below the limit of clinical detection. It is common for keratoconus to be diagnosed first in one eye and not until later in the other. At our hospital, we use a very sensitive Topography instrument called the ‘Topolyser’ from Wavelight Inc.
Progress
However good the vision may be with the use of contact lenses, vision may be difficult to maintain at times as the condition progresses and contact lens tolerance varies. Contact lenses are used as temporary measures of treatment, but do not, unfortunately, slow down the rate of progression of the cone. In about 10% to 20% of keratoconus patients the cornea may become extremely steep, thin and irregular or the vision cannot be improved sufficiently with contact lenses. The cornea may then need to be replaced surgically with a corneal transplant or graft. Visual recovery after a transplant takes a long time – sometimes as long as a year to 18 months – to settle down and there is a strong possibility that the eye will still need to be fitted with a contact lens afterwards in order to see properly. Surgery is therefore not a shortcut to perfect vision and nor is it a way of avoiding contact lens wear. There is also a risk of the transplant rejecting afterwards, although a majority of corneal transplants done for keratoconus are successful.
Keratoconus Treatment
Treatment of mild keratoconus is geared towards eliminating or reducing the myopia and astigmatism.
Temporary Treatment
Contact Lenses
Permanent Treatment
New modality of treatment: Corneal Collagen Crosslinking with Riboflavin (C3-R®*), CXL, New CSO-Vega
Temporary Treatment
Contact lenses
Nitial management is tried with rigid contact lenses by our contact lens specialist. In very early stages of keratoconus, spectacles can suffice to correct minor astigmatism. As the treatmentcondition progresses, spectacles may no longer provide the patient with a satisfactory degree of visual acuity, and most doctors will move to managing the condition with contact lenses.
Rigid gas permeable contact lenses for keratoconus improve vision by means of tear fluid filling the gap between the irregular corneal surface and the smooth regular inner surface of the contact lens, thereby creating the effect of a smoother cornea.

A new permanent non surgical treatment
Corneal collagen crosslinking with riboflavin (c3-r®*), cxl, cso-vega
So far there has been not one successful way to stop the progression of keratoconus.With current methods using rigid contact lens or intra corneal ring segments, only the refractive error (spectacle numbers) can be corrected, but it has very little effect on the progression of keratoconus. It is estimated that eventually 21% of the keratoconus patients require surgical intervention to restore corneal anatomy and eyesight. A new non surgical, non invasive treatment, based on collagen cross linking with Ultraviolet A (UVA, 365nm) and riboflavin (Vitamin B 2), a photosensitizing agent is now available. This changes the intrinsic biomechanical properties of the cornea, increasing its strength by almost 300%. This increase in corneal strength has shown to arrest the progression of keratoconus in numerous studies all over the world. What are the risks and consequences involved?
Very few potential risks associated with this treatment have been reported so far. The Ultraviolet light dose used is designed to prevent damage to the cells that line the back of the cornea or the other structures within the eye.
There is therefore discomfort and a short-term haze.
No lens opacities (cataracts) have been attributed to this treatment in European trials.
The treatment involves the outer layer (epithelium) of the cornea
Other lesser but more common risks include
- Inability to wear contact lenses for several weeks after the treatment
- Changes in corneal shape necessitates fitting of a contact lens or a occasional change in spectacle correction.
As is the case with any treatment, there may also be long-term risks that have not yet been identified. - The increased corneal rigidity induced may wear off over time and further periodic treatments may be required.
How does Cross Linking arrest keratoconus?
Until recently, there was no method to change the integrity and strength of the cornea itself for keratoconus patients. The non-invasive treatment C3-R®* (corneal collagen cross-linking riboflavin) treatment has been proven to strengthen the weak corneal structure in keratoconus. This method works by increasing collagen cross-linking, which are the natural “anchors” within the cornea. These anchors are responsible for preventing the cornea from bulging out and becoming steep and irregular (which is the cause of keratoconus). The figures above show the parallel corneal layers (white) and the collagen cross-linking (red) which increased after C3-R®* treatment
Are there any published studies for the same?
In published European studies, such treatments are proven safe and effective in patients. The 3 and 5 year results of Dresden clinical study in human eyes has shown arrest of progression of keratoconus in all treated eyes. (Wollensak G. Crosslinking treatment of progressive keratoconus: New Hope. Current Opinion in Ophthalmology 2006; 17: 356 – 360). Biomechanical measurements have shown an impressive increase in corneal rigidity of over 300% after crosslinking. The Dresden, Germany clinical study has shown that in all treated eyes the progression of keratoconus was stopped (‘freezing’). In over 53% of those eyes there was a slight reversal and flattening of the keratoconus by up to 2.87 diopters. Best corrected vision improved by 1.4 lines. This technique has shown great promise in treating early cases of the disease.
For glaucoma surgery
Do NOT use the dilating eye drops
For retinal / squint surgery if under g.a. (general anasthesia)
Fasting time should be 12 hours prior to time of surgery. Patient must not have any solid or liquids in this period except few sips of water to take any medications for high blood pressure, cardiac problems, asthma etc
For those on anticoagulant treatment
If you are using any anti coagulants like aspirin, Ecosprin, Loprin etc – Stop it 72 hours before the date of surgery. If using long acting anticoagulants such as Warfarin, Clopidogrel etc – Stop the tablets 7 days earlier. The same can be restarted the day after your surgery. If you have any further queries please call the hospital and speak to the Nurse for clarifications.

Activities to be expected after surgery
After the surgery you will be seen by the doctor and may go home shortly thereafter. You must not drive yourself home! Please make arrangements beforehand for a ride. 2. The day of surgery you should plan to take it easy. Generally there is very little if any discomfort following surgery. If you do experience some mild pain, you may take the pain killers prescribed. 3. Your eye will be patched after surgery. You will receive specific instructions at the end of surgery before your leave the hospital. The dark glasses/Protective glasses should be worn one the eye-pad is removed, generally in the same evening of the surgery. It is advised to wear protective glasses even at night and in bed for the first 2 days after surgery. This is to prevent accidential rubbing of the eye. You will be informed of all post operative care and instructions by the Nurse at time of discharge along with the discharge summary and list of post-op medicines. Improvement in vision is gradual. Glasses are generally prescribed within 1-3 weeks of surgery as per the healing. These glasses may need to be adjusted later as your eye continues to heal.
Any increase in redness or pain or sudden decrease in vision needs an urgent check-up with the doctor.
This may be a sign of serious infection in the eye
Specific post operative instructions
Cleaning your eye
For the first week following surgery you should protect the eye from injury. Do not rub or put pressure on the eye. Take small pieces of cotton wool and place them in a bowl containing water. Boil for 15 minutes and keep the bowl covered. Wash your hands with soap. Take a small piece of the sterilized cotton wool from the bowl. Squeeze out the excess water. Clean the discharge around the upper and lower lids without applying pressure on the eye. This is generally needed in the morning as long as the ointment is being used at bed time. Fresh cotton is to be boiled twice a day if needed.
Putting eye drops
Never use a pin/needle to open the eye drop bottle. Screw on the cap tight to open it. Retract the lower lid and instill one drop of the prescribed eye drop into the eye. Eye drops should be used as per the prescription. Only 1 drop at a time is enough. Keep both eyes closed for atleast 10 minutes after.
Rotecting your eyes
Each eye drop. Put on dark glasses throughout the day for one week. Wipe tears below the margin of the dark glasses. Do not touch the eye. Do not place cotton wool between the glasses and the eye. Do not sleep on the operated side for 2 days. For the first 5 days from the time of operation, take a bath below the neck. Face and hair can be washed after 5 days. But avoid getting water inside the eye.
Activities
Avoid strenuous activities.
Do not lift any objects heavier than 10 kg for about 5 days after the surgery
You may start reading and watching TV after 2 days. Take rest frequently with both eyes closed.
Many people return to light work immediately after surgery, but please discuss your needs with your doctor during your post operative visit (next day).
Ask your doctor about any specific activities you may have in mind as in leaving town, driving, yoga, walks, gym etc.
C3R Eye Treatment Cost?
Know the exact cost of C3R Eye LASIK and other Laser eye procedures that we have at our LASIK centre, Please fill the form or Call Our Customer Care.
Follow up visits
Please come for a post operative check up as advised upon discharge. Generally the next day, one week and one month post-op. As a routine all operated eyes should be checked once every six months even if you have no problem. If you have any further questions regarding your surgery or post operative treatment kindly speak to the Nurse who will coordinate with your doctor to answer your queries. Collagen Crosslinking treatment in one of the latest advancements in ophthalmology. Internationally launched at the ESCRS conference in London in September 2006.This treatment provides a ray of hope for lacs of Indian keratoconus patients.
C3R is a non-surgical procedure.
Only known procedure that is proven to halt the progression of the dreaded Keratoconus. This treatment now offers an end to a lifetime of waiting and uncertainty for Keratoconus patients. This is a simple one-time treatment that offers a permanent solution to Keratoconus. It does not require heavy precautions or regular follow-up visits, does not need an eye donor as required in ‘Corneal Transplant’, does not require any stitches or incisions in the eye, takes around one hour and the recovery is quick. This procedure is a boon for patients with keratoconus. Keratoconus is amongst the most dreaded of eye diseases, as in most of the cases, the disease progresses relentlessly during the young age, does not have any acute symptoms initially and thus is often not detected in the early stages.